| |
|
|
HERNIATION SYNDROMES |
|
Herniation is a neurologic emergency that requires
immediate intervention. Close monitoring, preferably by a
neurointensivist is required to help avoid neurological catastrophe. A
neurosurgical intervention may be necessary depending on the etiology of brain
herniation.
In order to understand the clinical aspects of brain
herniation syndromes, one must first appreciate the physiology. The
Monro-Kellie doctrine, proposed from
experiments from more than 200 years ago, discovered that in an adult, the sum
of the volumes of brain, blood and CSF are constant. An increase in one of these
three substances, requires a decrease in the volume of another.
(Brain parenchyma + CSF + Blood) volume = Constant volume
A main reason for the above phenomenon is that the cranial contents in adults
are enclosed (after fontanel closure) within a rigid, poorly compliant cranium
composed of bone and dura. Due to the poor compliance of this system, small
increases in intracranial volume will result in sharp increases in intracranial
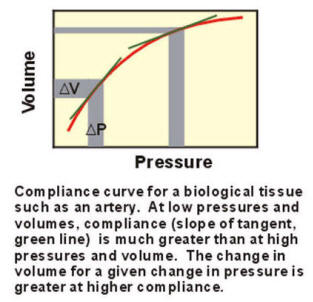
pressure. Compliance refers to the ratio of change in volume to change in
pressure.
C (compliance) =
Δ V (volume) / Δ P (pressure)
In most biological tissues, the relationship between change in volume to
change in pressure is not linear. Thus as demonstrated by the graph below, at
higher levels of volume, it requires a smaller change in volume to produce a
given change in pressure. |
|
 |
|
Any new masses developing within the cranial cavity, such as hematomas, tumors
or edema are initially tolerated by the minimal compliance of the brain.
However, after a very small increase of volume to the cranial contents, the
brain will displace due to a very large increase in intracranial pressure (ICP).
The tissue may displace one brain compartment into another. The physical
movement of brain tissue, if not recognized and treated urgently, compromises
vital structures and may result in brain death due to irreversible brainstem
dysfunction or disruption of respiratory and cardiovascular centers resulting in
death from respiratory or cardiac arrest. |
|
|
|
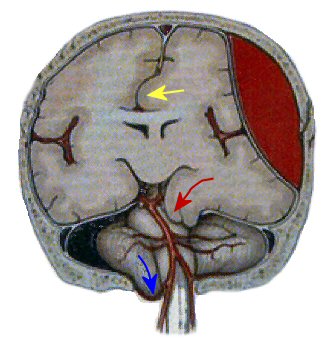 |
Above: Herniation syndromes. Red arrow - Transtentorial (uncal) herniation; Blue arrow
- Foramen magnum herniation;
Yellow arrow - Subfalcine herniation
|
Transtentorial Herniation
|
|
|
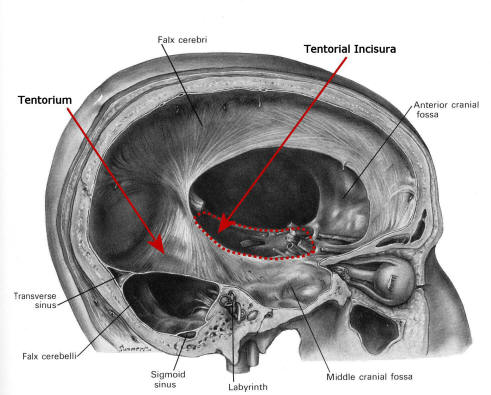
The tentorium is a dural structure that
separates the cerebrum from the brainstem and cerebellum in the posterior
cranial fossa below. The opening in the tentorium through which the brainstem,
specifically the midbrain, connects to the cerebrum is the
tentorial incisura. The presence of a large
supratentorial mass in one hemisphere often results in
subfalcine herniation, where the cingulate gyrus of the ipsilateral
hemisphere is compressed and herniates under the falx to compress the
contralateral hemisphere. Subsequently, progression of the herniation then
becomes transtentorial with the supratentorial contents moving through the
tentorial incisura.
|
|
 |
Above: Uncal herniation. Arrows point to the
medial temporal lobe that has herniated through the tentorial incisura to
compress the midbrain
|
The structure that herniates first is usually the uncus
on the medial temporal lobe. As the uncus herniates, it first presses against
the midbrain, resulting in an ipsilateral third nerve palsy. As the
parasympathetic fibers are on the outside of the third nerve, the
first sign of uncal herniation is usually pupillary
dilation. Further compression results in paralysis of extraocular
muscles.
Because transtentorial herniation occurs most commonly from a
supratentorial mass, the patient usually will already have a contralateral
hemiplegia. If the brainstem is torqued, the contralateral cerebral peduncle can
be compressed against the tentorial notch (i.e.,
Kernohan’s notch), resulting in quadriplegia (contralateral
hemiplegia from the initial lesion, ipsilateral hemiplegia from Kernohan’s notch
phenomena). As herniation proceeds, dysfunction of both hemispheres occurs
followed by dysfunction of the brainstem. As this occurs, abnormal posturing is
seen.
|
|
|
|
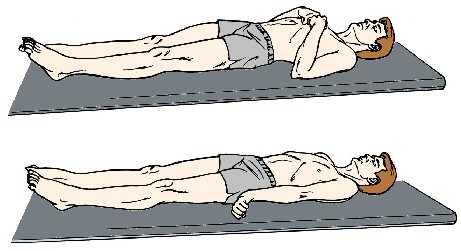
Decorticate posturing (figure top) is
recognized as bilateral flexion at the elbows and wrists, shoulder adduction and
extension of the lower extremities occurring with lesions above the midbrain’s
red nucleus. As brainstem dysfunction proceeds inferiorly,
decerebrate posturing (figure bottom)
occurs, recognized as rigid extension of the arms with internal rotation, and
extension of the legs with internal rotation and downward pointing of the toes.
Retraction (backward arching) of the head may occur. This is followed by
respiratory insufficiency and death.
|
|
|
|
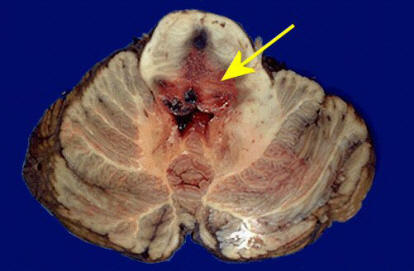
Above: Duret hemorrhages.
These are the terminal event in transtentorial herniation. |
|
Pathologically, the downward herniation stretches the penetrating branches of
the basilar artery, which then rupture, causing secondary linear hemorrhages in
the midbrain and pons, known as Duret hemorrhages.
These are generally fatal.
Also passing through the tentorial incisura are both posterior cerebral arteries
(PCA). Although deficits secondary to PCA ischemia are difficult if not
impossible to determine clinically at the time; patients who survive an episode
of transtenorial herniation may be left with bilateral PCA infarcts (i.e.,
cortical blindness or other bilateral visual field abnormalities; and marked
short term memory dysfunction from involvement of the medial temporal lobes).
|
|
Foramen Magnum Herniation
Foramen magnum herniation occurs from either a posterior fossa space-occupying
lesion or from further progression of a supratentorial mass lesion. Foramen
magnum herniation causes compression of structures that lie above and pass
through the foramen magnum, (i.e., the cerebellar tonsils and medulla). In the
medulla are located the vital centers regulating respiration and cardiac
function, and the reticular activating system for maintaining consciousness. In
foramen magnum herniation, the following develop: changes in the level of
consciousness, extensor posturing, apnea, and then circulatory collapse followed
by death.
|
|
|
|
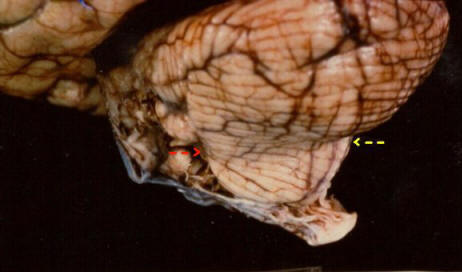
Above: Pathologic specimen of foramen magnum
herniation. Below the arrows mark where the cerebellum had herniated downwards
into the foramen magnum, resulting in compression of the medulla. |
|

|
|
Above: Herniation of the cerebellar tonsils
(red arrow) and compression of the medulla. The dotted white line shows the level
of the foramen magnum. |
|
|
|