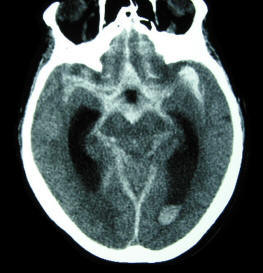
Definition
Subarachnoid hemorrhage (SAH) is the extravasation of blood into the
subarachnoid space between the pial and arachnoid membranes.
Etiology
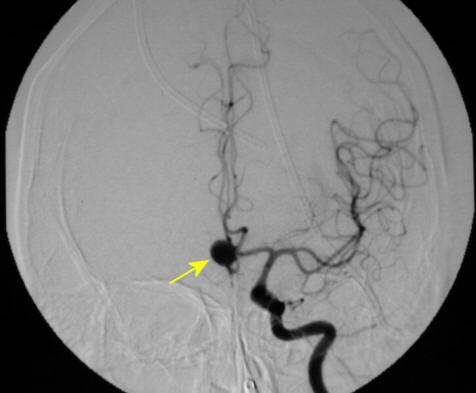
The most common causes of spontaneous SAH are rupture of saccular, or berry,
aneurysm (80%); and rupture of arteriovenous malformation (AVM) (10%).
Other causes of non-traumatic SAH include: mycotic aneurysms, amyloid
angiopathy, blood dyscrasias, fibromuscular dysplasia, idiopathic, infection,
Moyamoya disease, neoplasm, and vasculitis (10%).
Epidemiology (Frequency, Age, Sex, Race)
Unlike other subcategories of stroke, the incidence of SAH has not decreased
over time. However, since 1970, survival rates have improved. Annual incidence
of aneurysmal SAH worldwide varies from 2-49 cases per 100,000 population, with
the highest rates occurring in Japan and Finland. Annual incidence of aneurysmal
SAH in the United States is 6-16 cases per 100,000 population, with
approximately 30,000 episodes occurring each year. Incidence peaks at age 50.
There is a 3:2 female to male ratio; and a 2:1 black to white ratio.
Incidence of SAH from aneurysmal and AVM rupture is significantly higher during
pregnancy, especially the third trimester. SAH from aneurysmal rupture accounts
for 6-25% of maternal deaths during pregnancy.
Aneurysm Pathophysiology
Aneurysms are specific to the intracranial arteries because their walls lack
an external elastic lamina, they contain a very thin adventitia, and they lie
unsupported in the subarachnoid space.
The early precursors of aneurysms are small outpouchings through defects in the
media of the arteries. These defects expand as a result of hydrostatic pressure
from pulsatile blood flow and blood turbulence. A mature aneurysm has a paucity
of media, replaced by connective tissue, and has diminished or absent elastic
lamina.
The probability of rupture is related to the tension on the aneurysm wall, as
determined by the Law of La Place; thus, the rate of rupture is directly related
to the size of the aneurysm.
Aneurysms with a diameter of 5
mm or less have a 2% risk of rupture
Aneurysms with a diameter of 6-10 mm have a 40% risk of rupture
Aneurysms usually occur at arterial bifurcations
Aneurysms mostly arise from the anterior circulation of the Circle of Willis
(85%)
The
Most
Common Sites of Aneurysms are:
Internal carotid
artery/posterior communicating artery (41%)
Anterior communicating
artery/anterior cerebral artery (34%)
Middle cerebral artery (20%)
Vertebral artery/basilar artery
(4%)
Other arteries (1%)
Aneurysm Formation
Acquired factors associated with aneurysm formation include:
Atherosclerosis
Hypertension
Hemodynamic stress
Evidence supporting the association between congenital factors and aneurysm
formation:
Clusters of familial occurrence
(e.g., in Finland, the incidence of familial cerebral aneurysm is 10%)
Incidence of multiple aneurysms
in patients with SAH (15-20%)
Association with specific
congenital diseases (e.g., coarctation of the aorta, Marfan syndrome, Ehlers-Danlos
syndrome, fibromuscular dysplasia, polycystic kidney disease)
Known Risk Factors for Aneurysm Rupture
Tobacco use
Alcohol abuse
Hypertension caused by cocaine
and other stimulants
Large aneurysm size
Prodromal Signs and Symptoms
Prodromal signs and symptoms
are the result of sentinel leaks, mass effect of aneurysm expansion, or emboli.
Sentinel, or "warning," leaks
that produce minor blood leakage are reported to occur in 30-50% of aneurysmal
SAHs; they do not usually occur in the setting of AVM.
Sentinel leaks produce sudden
focal or generalized head pain that may be severe; they also produce nausea,
vomiting, photophobia, malaise, or, less commonly, neck pain.
Sentinel headaches precede
aneurysm rupture by a few hours to a few months, with a reported mean of 2 weeks
prior to discovery of the SAH.
Mass effect of an expanding
aneurysm has characteristic features based upon aneurysm location. The most
classic is an ipsilateral 3rd nerve palsy from a Posterior Communicating Artery
aneurysm.
Transient ischemic attacks can
occur from emboli originating from intra-aneurysmal thrombus formation.
Signs and Symptoms of Aneurysmal Rupture
A sudden onset of
severe
headache ("thunderclap headache"), often described as the
“worst headache of my
life;” absence of headache in the setting of a ruptured aneurysm is rare.
Nuchal pain and rigidity, back
pain, and bilateral leg pain secondary to meningeal irritation occurs in as many
as 80% of patients, but may take several hours to manifest
A sudden loss of consciousness
(LOC) occurs in half of patients at bleeding onset; it is usually transient,
although 10% of patients are comatose for several days
Nausea and/or vomiting
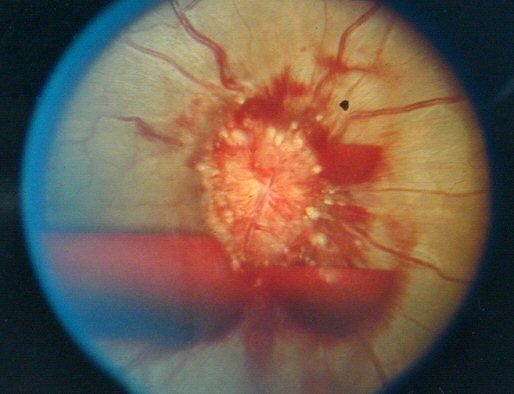
Photophobia and/or visual
disturbances
Seizures occur in 10-25% of
patients, usually in the first few minutes after bleeding onset
Less severe hemorrhages may
present with headache of moderate intensity, neck pain, and nonspecific symptoms
Approximately 30-40% of
patients are at rest at the time of SAH
|