|
Upper Motor Neuron Lesions
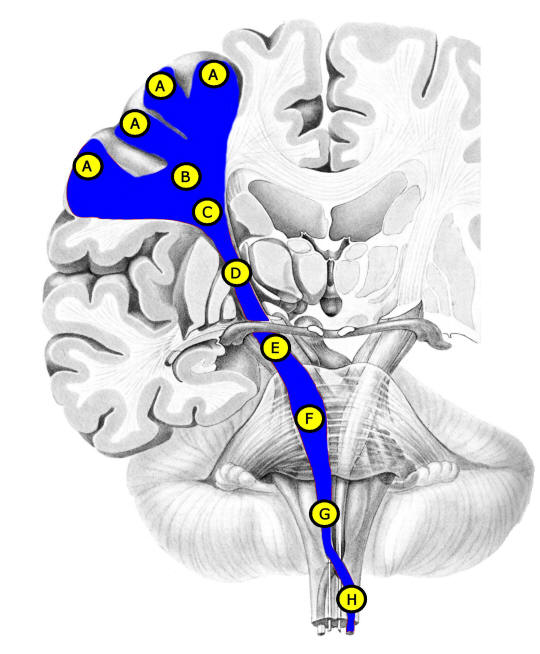
• Anatomy. Cell bodies of the primary
motor cortex are located in the
precentral gyrus (A)
of the frontal lobe. Axons travel in the deep white matter (centrum
semiovale (B) and corona radiata (C)),
internal capsule (D),
cerebral peduncle (E) (midbrain), basis pontis
(F)
(pons), and pyramids (G) (medulla). Most of the
fibers cross in the caudal medulla, and proceed down lateral corticospinal
tracts (H) in the contralateral spinal cord
prior to synapsing at segmental
levels on the lower motor neurons.
• UMN Syndrome. Lesion of either the cell body or (more commonly) the axon can produce
a characteristic UMN syndrome. To localize to a specific part of the brain or cord, the clinician must
use other clues, usually derived from collateral damage sustained by nearby
structures serving other functions. The UMN syndrome consists of the following:
Weakness. The weakness may vary from subtle (mild coordination disturbance)
to severe. The weakness has a characteristic pattern: in the upper extremities,
elbow extension is weaker than flexion; wrist extension is weaker than flexion;
and shoulder abduction is weaker than adduction.
In the lower extremities, the hip abduction is
weaker than adduction; knee flexion is weaker than extension; ankle dorsiflexion is weaker than plantarflexion; and ankle eversion is weaker than
inversion. In addition, most UMN lesions tend to cause more severe weakness
distally.
Hyperreflexia. All the muscle stretch reflexes are increased. Abnormal
hyperreflexia can be determined by comparison to the contralateral side (for
unilateral lesions), or if there is clonus or pathologic spread of reflexes
(e.g., tapping on the ankle reflex results in hip adduction as well).
However, it is important to note that severe or acute UMN lesions may result in
hyporeflexia initially. This is known as cerebral or spinal shock. Only days or
weeks later does hyperreflexia develop.
Spasticity.
Spasticity is a type of increased muscle tone (resistance to
passive movement). In spasticity, the tone increases as the limb is moved rapidly. If
the limb is moved slowly enough, the tone increase is not apparent. The
phenomenon of spastic “catch” reflects this behavior. Spasticity
also displays a "clasped knife" type of feel - initially there is increased tone
which then gives way as the limb is moved (similar to opening a
clasped knife). When testing muscle tone, it is usually increased in the flexors
of the upper extremity and the extensors of the lower extremity. However, similar to reflexes above, UMN
lesions may initially display decreased tone or flaccidity. Again, it is only
days or weeks later that spasticity develops in an UMN lesion.
|