|
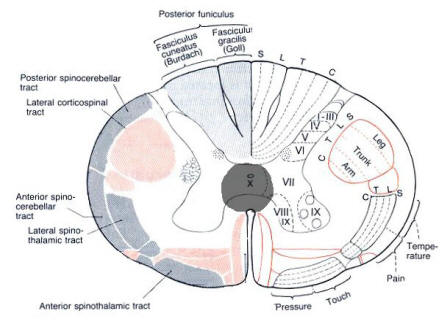
The initial signs and symptoms caused by central cord lesion are often related to dysfunction of
the fibers that pass through the anterior
white commissure (i.e., the crossing spinothalamic tracts
at that level). This
results in a cape-like distribution of decreased sensation to pin and
temperature at the level of the lesion. Motor function as well as
vibration is preserved in small lesions.
Further symptoms are caused if the lesion expands into additional cord regions. Lesions
that include the anterior gray matter of the spinal cord may destroy the
anterior horn cells, causing weakness and wasting of muscles (lower motor neuron
signs) at the involved levels. Further enlargement of the area of the lesion may
result in involvement of the spinothalamic tracts. Because spinothalamic tract
fibers serving the sacral areas travel most superficially in the spinal cord, an expanding
central cord lesions will cause increasing areas of
anesthesia, but with a tendency spare the sacral area, as these fibers are most
distant from the center of the cord. Thus, an expanding cervical
central cord lesion may begin by causing an area of cape-like anesthesia
involving the arms but with progressively descending sensory involvement to the
point that only the saddle area is spared ("sacral
sparing").
The most common causes of such central lesions are syringomyelia, intrinsic cord tumors,
trauma, and demyelination. |