| |
|
|
CLINICAL PRESENTATION OF CEREBELLAR DISEASE |
|

|
The cerebellum connects widely in the neuraxis (brainstem, spinal cord, and
nearly all areas of the cerebral cortex) to aid in coordinating voluntary
movement. The cerebellum also plays a key role in balance and eye movements.
Clinically, disorders of the cerebellum can be divided into those that affect
the hemispheres, and those at the affect midline structures, the latter
including the vermis and the floculonodular lobe. |
Clinical Signs of Disease in the Cerebellar
Hemispheres
A lesion in one cerebellar hemisphere will cause motor deficits on the
ipsilateral side of the body. This is due to
the “double cross” (i.e., input fibers cross
to reach the cerebellum, and cerebellar output fibers cross to reach their
destination). In general a lesion in the cerebellar hemisphere results in a
deterioration of coordinated movements, or a decomposition of movement. The
cerebellar hemispheres influence the planning and control of precise movements
of the extremities and in the timing of these movements. |
|
• Dysmetria. Patients will
past-point (i.e., reach past a target, or fall
short of the target) |
|

|
|
• Tremor.
The tremor in cerebellar disorders is an action
intention tremor (i.e., it is brought out by voluntary movement).
Characteristically, the tremor is 1) more pronounced as the patient approaches
the endpoint; 2) is a
proximal tremor (i.e., affects the shoulder and
hip girdles muscles predominantly); and 3) the direction of the tremor is
perpendicular to the movement of the limb.
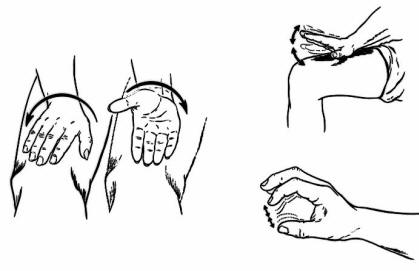
Tremor is test with the finger-to-nose and heel-to-skin (see figure above)
tests. Note that at rest there will be little or no tremor. |
|
|
|
•
Dysdiadochokinesia (a.k.a., impaired rapid alternating movements).
There will be fragmentation and slowing of the movement as well as inaccuracy
when performing rapid alternating movements (see figure above).
• Rebound
phenomena. This is also known as an impaired check, or an inability
of muscles to adapt to rapid changes in load. For example, if the patient is
pushing against the doctor's hand and then the hand is pulled away unexpectedly,
the patient's arm will overshoot where it would normally stop.
• Dysarthria.
The speech is described a scanning. It is
essentially ataxia of speech. Often the pitch or rhythm of the speech will
change. Grammar and word usage will still be correct.
• Nystagmus.
Patients often display nystagmus, often bilateral.
• Unsteady
gait. Patients will have an unsteady gait and a tendency to lean or
even fall to the side of the lesion. This will be due to ataxia involving the
lower extremities (not the truncal ataxia with vermis lesions (see below). |
Clinical Signs of Disease in the Cerebellar Vermis,
Including the Floculonodular Lobe:
Lesions to this section of the cerebellar midline will result in bilateral
deficits. The structures of the vermis influence posture, balance, and
equilibrium. This occurs through the vestibulospinal and reticulospinal
projections to extensor motor neurons of the axial and proximal limb muscles. |
|
• Severe Gait
Ataxia. The patient will have an unsteady, lurching gait. The patient
may have exaggerated movement of the legs and a tendency to fall to the side,
forward, or backward. The stance itself will be wide-based. This patient will be
unable to do a tandem gait (heel-toe-heel-toe), walk on their heels, or walk on
their toes.
• Titubation.
This is essentially a tremor of the axial body or head. This can be as severe as
causing the patient to be unable to sit or stand unsupported.
• Nystagmus.
This is most prominent especially if the flocculonodular lobe is involved. If
present, it will be maximal towards the side of the lesion. |
Nonspecific Findings Associated with Cerebellar
Lesions
• Hypotonia.
on the ipsilateral side (this is often mild or difficult to appreciate)
• Vomiting.
Vomiting can be seen in both disease of the vermis and of the hemispheres. In
this setting, the characteristics of the vomiting are important, particularly
with cerebellar tumors. There are three "P's" of vomiting with cerebellar
disease: 1) Postural. Patients will complain of vomiting associated with a
certain position; 2) Positional. Patients will note that suddenly changing
position, particularly when sitting up quickly, brings on the vomiting; and 3)
Projectile. Often, the vomiting occurs very suddenly without nausea and thus
tends to be projectile. |
|
|
|