| |
|
|
EXTERNAL COMPRESSION OF THE
SPINAL CORD |
|
|
|

|
Lesions that compress the spinal cord from an outside location are among the
most important and sometimes the most difficult to diagnosis. Extrinsic
compressive lesions often disrupt the motor and sensory roots at the level of the
lesion. This results in a lower motor neuron syndrome at the level of the lesion
(i.e., a radiculopathy).
|
|
 |
|
External lesions that compress the spinal cord produce symptoms in the
most superficial fibers of the long pathways first. Owing to the
specific lamination of the corticospinal and spinothalamic tracts
(lower extremity fibers most superficial and upper extremity fibers
deepest), cervical compressive lesions may cause sensory and motor symptoms to
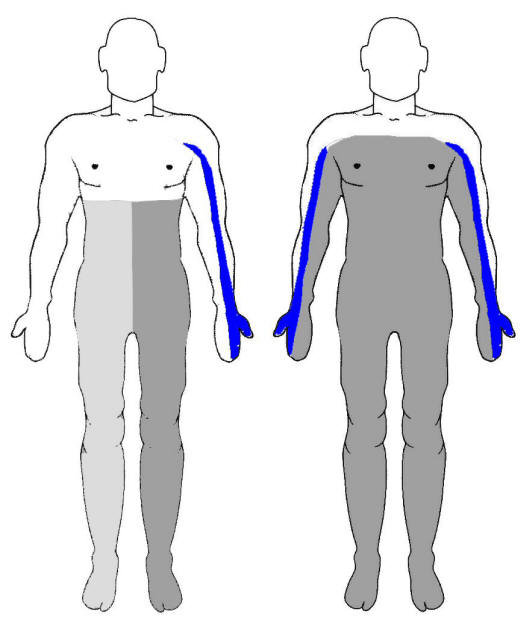
appear first in the lower extremities. Thus, a common early pattern is a
radiculopathy at the level of the compression along with sensory and motor
symptoms in the distal lower extremities (see figure above - left: (blue)
radicular symptoms; (dark gray) spinal cord symptoms). Symptoms may then appear to "ascend" as
the compression becomes more severe and more deeply situated fibers are
successively affected. This anatomical arrangement is notorious for the
production of falsely localizing levels. For example, a distinct level of sensory
loss may be discernible at the level of the umbilicus (T10) in the case of a
compressive tumor at the mid-cervical region (see figure above - right). The unwary clinician obtaining a
magnetic resonance imaging scan of the thoracic cord might be falsely reassured
by a normal result because the level of the spinal cord where the lesion is
located is not imaged.
Therefore, the level of a sensory deficit found on
examination produced by extrinsic, compressive cord lesions only marks the
lowest possible level of the lesion; the actual pathology may lie anywhere
between the level of sensory loss and the foramen magnum. Identification of a
root level can be a very helpful sign; the upper limits of a sensory (or motor)
level found on examination only marks the lowest possible location of the lesion
in the spinal cord for the reasons described above. When, in addition, a focus
of back pain is present or distinct lower motor neuron signs are found at a
specific level, the level of the lesion may be pinpointed. Likewise, localized
pain or tenderness over a vertebral spinous
process may help localize a process associated with a destructive bony lesion. |
|
 |
|
Lateral compressive lesions, though not causing a spinal cord hemisection per
se, may resemble the Brown-Séquard syndrome in presentation
(see figure above left). Except in the case
of early lesions, there is often some bilaterality to signs and symptoms with
lateral compressive lesions of the cord, especially when the contralateral cord
becomes compressed against the opposite side of the spinal canal. In cases of
lateral compression rather than hemisection, the half of the spinal cord
ipsilateral to the compressive lesion is usually more symptomatic than the
contralateral half. In the late stage of external spinal cord compression, the
syndrome evolves into a complete transection
with upper motor neuron paralysis and numbness below the lesion, and a segmental
lower motor neuron syndrome at the level of the lesion (see figure above -
right). |
|
|
|